




June 24, 2026
Article
Overview
The 2026/27 GP contract introduces further changes to funding, workforce and delivery expectations. While the overall funding position has improved in cash terms, it is static in real terms, meaning practices will need to plan carefully to protect profitability and manage workload.
Headline Funding
The contract delivers £485 million of additional investment across the core contract and Network DES, equating to 3.6% cash growth (1.4% real terms). At best this uplift will offset rising staff costs and inflation and but is unlikely to give practices the resources they feel they need to facilitate constant online access, uncapped advice and guidance and same day urgent care requirements.
Core Contract Changes
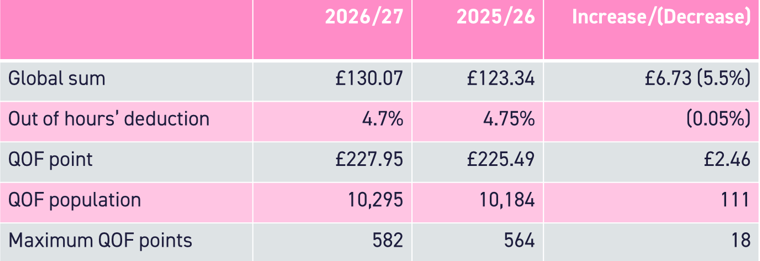
The global sum increases to £130.07 per weighted patient (5.5% uplift), and the Out of Hours opt out has reduced from 4.75% to 4.7%. While this provides a welcome boost to income, practices should note much of this increase reflects embedded pay uplifts advice and guidance, rather than new discretionary funding.
QOF sees the addition of 18 new points with a focus on obesity and preventative care with improvement targets for childhood immunisations alongside the % population target. The value of a QOF point has increased to £227.95, however population adjustments mean there is little overall financial gain.
The Advice and Guidance enhanced service introduced in 2025/26 has been retired and moved into the core contract. Practices are expected to use it routinely where clinically appropriate using local referral pathways. This will undoubtedly increase clinical and administrative workload.
Locum reimbursements have increased inline with the DDRB uplift of 3.5%.
GP Reimbursement Scheme
A key structural change is the introduction of the GP Reimbursement Scheme.
The purpose of the funding is to increase GP capacity to support clinically urgent same day access, but it is not new money. The scheme replaces the Capacity and Access (CAP) fund previously paid to PCNs.
Practices can claim for newly employed salaried GPs and existing salaried GPs increasing sessions up to a maximum of 9. GPs already in employment that were previously funded using CAP can continue to be claimed for under this GP reimbursement scheme.
Key considerations:
- Reimbursement is capped at £4.57 per adjusted patient per practice
- The maximum claim is £152,900 for a FTE GP (FT being 9 sessions!) so allows for circa £12,500 per session after on costs
- Applies to salaried GPs only. It cannot be used for locums or absence cover.
- Newly employed Salaried GPs cannot have worked for the practice in the previous 12 months, unless they came in to provide cover or have since retired
- Contractors with more than 3,500 patients per GP must get NHSE approval
- Practices can transfer their entitlement to another practice in the PCN
The change represents a shift away from a flexible income stream that PCNs and practices were using to improve access in different ways, to a restrictive scheme that only covers salaried GP costs. Those that were using CAP to fund software, locums or other costs will need to think carefully about how to fund those costs for the year ahead.
The change continues the trend of moving to a reimbursement model. Practices now have to spend the money before being reimbursed which could have an adverse effect on practice/PCN cashflow and may increase the working capital requirement.
It is also worth noting that the scheme is not guaranteed beyond 31 March 2027, so practices need to take care when employing new GPs. Upcoming changes to employment legislation also mean that care needs to be taken with fixed term contracts, and potential redundancy liabilities need to be considered when a fixed contract comes to an end.
PCN Network DES Changes
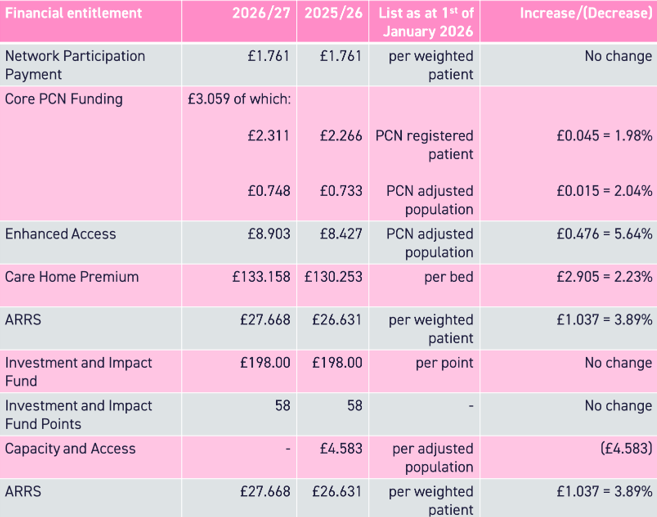
PCN funding remains largely static in real terms. The removal of Capacity and Access funding creates a significant gap for PCNs that previously used this to support shared services.
ARRS rules have been relaxed to allow greater flexibility in GP recruitment. From 1 April the scheme is open to all GPs, not only those that are newly qualified. The maximum reimbursement has been increased to £152,900 to reflect that. However, the overall funding envelope has not increased so this will not allow for PCNs that were already utilising their total ARRS pot to increase GP capacity.
Local DES Flexibility and Neighbourhoods
ICBs can now introduce local variations to the Network DES with approval from NHS England. Changes must be agreed by all member practices and can be applied to service requirements and funding.
This provides an opportunity to align services with population need and implement Neighbourhood services ahead of the introduction of the new Neighbourhood contracts.
The first local variation in the country has recently been approved in Kent. This example brings £10m of new funding to general practice for services to complex and frail patients to reduce hospital admissions. This came after they identified that whilst this cohort made up only 5% of the population, they accounted for 30% of the hospital admissions, often ending up in longer than average stays.
PCNs need to be talking to their ICBs about Neighbourhood plans. These local variations and the new single and multi neighbourhood provider contracts (SNP and MNP) represent an opportunity for newly funded services, but also a threat that non-core services will be moved into new contracts that general practice is not in control of.
Carr-Hill Review
A review of the Carr-Hill formula is underway. The model is 25 years old and based on outdated data. It is widely recognised that it does not reflect multi morbidity, deprivation, frailty and access demand.
How the model will be changed is yet to be determined. It could involve a completely new model based on workload, or it could simply adjust the weightings with current data. Any change will bring winners and losers and could see the return of the Minimum Practice Income Guarantee (MPIG).
Whilst the new model is unknown, practices should start to consider their current weighting and population deprivation to understand the possible financial impact of any potential changes.
Summary
In reality, the 2026/27 contract increases workload in general practice without a significant uplift in funding. Practices will need to compare the income uplifts against cost increases to see what impact this has on practice profitability and partner drawings.
With the changes to workforce funding, practices should consider a short and medium term workforce strategy that delivers the services needed, reduces workload and allows the practices to operate profitably.
Practices will also need to assess the cashflow impact following the change from CAP to the GP reimbursement scheme and consider if the working capital in the business is sufficient.
All of these short term changes make it very difficult for practices and PCNs to get out of the weeds and consider how they want to shape the future of their Neighbourhood. But being in the conversation about local contract variations and any new Neighbourhood contracts will be necessary to maintain some control or influence over the future.
If you need support when considering what the contract changes mean for your practice/PCN, or aren’t sure what your next steps are when it comes to Neighbourhood working, then please do get in touch.